delta dental appeal form
Theres no hassle in working through claims saving you time and frustration. Gender M F 14.

Delta Dental
Delta Dental Premier Network Forms - Professional Application Credentialing form Delta Dental Premier Dentists Agreement Ownership Control Form and W-9.
. Use this secure form to file a grievance or appeal a dental benefits decision. Sale of Practice Notification Form. You can file a grievance by doing one of the following.
THE PO BOX IS FOR CLAIMS ONLY. Through our national network of Delta Dental companies we offer dental coverage in all 50 states Puerto Rico and other US. Delta Dental of Ohio is a part of Delta Dental Plans Association.
Sell ACA Dental plans on the Healthcare Exchange Agencies must complete an Appointment Form and Agent Fee Agreement for each agent that will sell solicit or negotiate business for Delta Dental of Arkansas. This form should only be used to submit an appeal. Locum Tenens Provider Form.
Disputes must be written and must clearly describe the basis of the dispute. Delta Dental HIPAA Form 14b ASO Groups. Delta Dental PPO and Delta Dental Premier network dentists submit claim forms automatically on behalf of Delta Dental patients.
If you wish to file a dispute with Delta Dental please complete the form below include all supporting documentation and clearly identify why you are disputing Delta Dentals action or inaction. Healthy Smile Healthy You enrollment form. Dental plans provided by Oregon Dental Service ODS dba Delta Dental Plan of Oregon and Delta Dental of Alaska.
Appeal Form - Information on how to appeal your claim. Automatic bank draft authorization for risk groups. Group Plan Appeals.
For changes regarding EFT please visit Dental Office Toolkit. Delta Dental of Arkansas. Through our national network of Delta Dental companies we offer dental coverage in all 50 states Puerto Rico and other US.
We have 1 business day after we receive the information from the treating provider to decide whether we should change our decision and authorize your requested service. Delta Dental of Arizona. Through our national network of Delta Dental companies we offer dental coverage in all 50 states Puerto Rico and other US.
Disputes not submitted on this form or lacking necessary information to resolve. Dentist Directory Update Form. Appeal Request Form and Instructions Providers or members who wish to file a formal appeal related to an adverse benefit determination must complete the Delta Dental of Kansas Appeal Request Form.
We cover more Americans than any other dental benefits provider - and strive to make dental coverage more accessible and affordable to a wide variety of employers groups and individuals. Delta Dental of Kentucky. Continuous Orthodontic Coverage Form for DeltaCare USA.
Dentist Change Request Form. CLAIMS APPEALS SENT TO THE PO BOX WILL BE DELAYED. Register a Super User for your office today.
The information provided on this site is for general education purposes only and is not intended as a diagnosis treatment or a substitute for professional medical or dental advice diagnosis or treatment. Appeals and Grievances PO. Delta Dental of Michigan is a part of Delta Dental Plans Association.
How To Appeal A Claim Claim Appeal Information. Healthy Smile Healthy You enrollment form Spanish. Box 6247 Sherwood AR 72124.
Gender M F M F U. Delta Dental of Washington is a part of Delta Dental Plans Association. Please refer to the vision appeals packet for information on submitting DeltaVision Administered by EyeMed appeals.
Please return completed forms by fax to 501-992-1899 or mail to PO. CLAIMS APPEALS SHOULD BE SENT TO THE STREET ADDRESS BELOW NOT THE PO BOX. PO Box 9219.
Removable Prosthodontics Assessment Form. Delta Dental PPO participation packet request. Delta Dental is Americas largest and most trusted dental benefits carrier.
Through our national network of Delta Dental companies we offer dental coverage in. Delta Dental of Oregon is a part of Delta Dental Plans Association. Box 15965 Little Rock AR 72231.
Farmington Hills MI 48333-9219. Call toll-free at 1-866-864-2499. Delta Dental of Minnesota provider forms for claims and remittance dental office support participation agreements and government programs.
Send a fax to 1-833-866-4650. If you need to add a provider remove a provider or notify us of a location change please complete the form below. Group Information Change Request Form.
You can download this form insert the necessary information and print it or you can print it and fill in the applicable information. Through our national network of Delta Dental companies we offer dental coverage in all 50 states Puerto Rico and other US. The Appeal Request Form must be received by Delta Dental of Kansas within 180 calendar days from the.
DeltaCare USA participation packet request. Thank you for being a participating provider. Delta Dental Smiles Attn.
ASO contract addendum for HIPAA privacy and security. How Do I File a Grievance. Delta Dental HIPAA Form 14a Risk Groups.
Dental Automatic Payment Form Online Access Administrator Role Direct Electronic Access Agreement Return completed form to your Account Executive Student Certification Form Use this form to certify dependents as college students Group Data Form Authorization To Release Protected Health Information Certificate Of Coverage For Small Businesses. With Delta Dental we keep you smiling. Re-Evaluation Committee 111 Shuman Blvd.
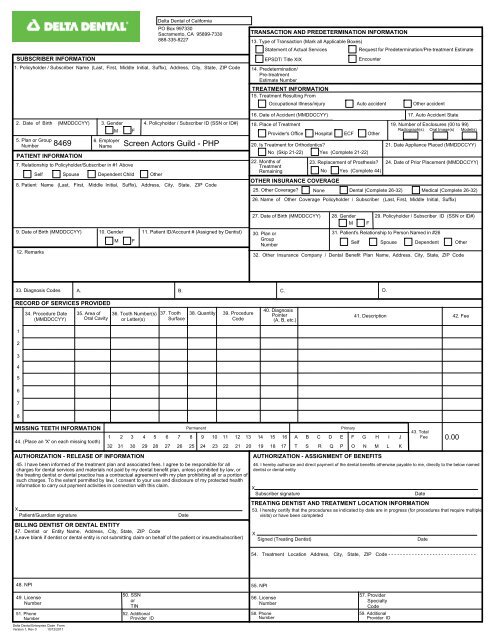
Group Claim Form This claim form is for Delta Dental PPO Delta Dental Premier and non-network claims.
Delta Dental

Pin On Teaching Teeth To Kids
Delta Dental

Claim And Admin Forms Delta Dental
2
2

Dental Health Tips From Infancy To Adulthood With Arm Hammer In Mar 2022 Ourfamilyworld Com Dental Health Health Tips Health Habits

Delta Dental
2

Delta Dental

Dental Insurance Forms Delta Dental Of Washington

Form Schedule K 1 38 Beneficiary S Share Of North Dakota Income Loss Flipping Houses Image Search Dental

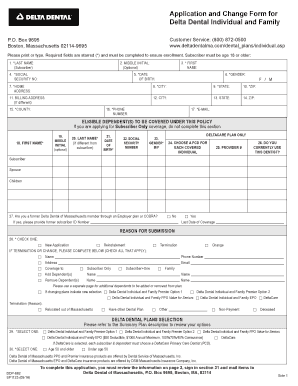
Fillable Online Disabled Dependent Application Delta Dental Massachusetts Form Fax Email Print Pdffiller
News Release Delta Dental Of Wisconsin
Delta Dental Ppo Ucnet University Of California

Delta Dental Contact Information Address
Delta Dental Individual Family Plans For 2019
2

News Release Delta Dental Of Wisconsin